
Treatment of Intersex Infants
Additional chapters in This Section include:
Gender Reassignment Surgery
Orchiectomy for MTF Transsexual Women
FFS Facial Feminization Surgery
MTF Transsexual Surgeries
Hormone Replacement Therapy for Transgender Women
Female Hormone Therapy MTF Transsexuals
Breast Development in MTF Transsexuals
MTF Transsexual Breast Enlargement
Breast Augmentation MTF Transsexuals
Lactation and the Transsexual Woman
Injecting Silicone for Transsexual Women
Brazilian Hips and Buttock Enlargement
Average Body Size MTF Transgender
Male and Female Skeleton Transsexuals
Treatment of Young Transsexuals
Puberty in Adolescents MTF Transgender
Treatment of Young MTF Transsexuals
Treatment of Intersex Infants
Androgen Insensitivity Syndrome
Female Physical Beauty Transgender
Transgender Female Beauty
Exercise, Fitness and Diet for Transsexual Women
Important |
Note: the speculations on this page are my own, and not those of the Intersex Society of North America (
ISNA
) or any other intersex support group.
When I established this page in 2000 it soon incorporated feedback from various community sources, nevertheless in May/June 2003 I was bombarded by emails from several ladies who
strongly
objected to this page. I was annoyed by the implication in some communications that only intersex individuals should write about the intersex condition, but nevertheless I took the page down. However after several supportive discussions I have resurrected this page for information purposes, minus some items. I would like comments from anyone mentioned on this page, and particularly welcome constructive feedback. I'm trying hard to strike a balance here.
|
Introduction
It is necessary to distinguish between intersex infants, and gender dysphoric (transsexual) children who consciously reject the gender in which they are being brought up.
An intersex (sometimes referred to as intersexual) infant is a baby born with ambiguous genitalia and sexual organs, neither clearly male nor clearly female. Many sources restrict to the definition to only "ambiguous external genitalia" but this excludes intersex children where their external genitalia are normal in appearance, for example in cases of complete Androgen Insensitivity Syndrome ( |
AIS
). I'm adopting the wider definition in this article.
Medically, intersex children can be categorised in to several main groups:
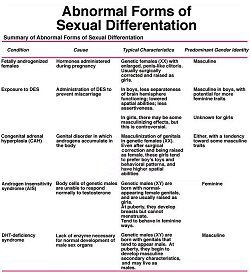
| True hermaphroditism - children who have both sex's internal reproductive organs. |
| Gonadal dysgenesis - children who have internal sex organs that are usually female but external genitals that may vary between normal female and normal male, with the majority female. |
| Pure gonadal dysgenesis - a female child who has underdeveloped gonads, internal female reproductive organs and female external genitalia. |
| Pseudohermaphroditism - children who have questionable external genitalia, but have only one gender's internal reproductive organs. |
Intersex infants have no say in their eventual sex and gender assignment, which in some cases may be contrary to their genetic karyotype (chromosomal sex).
|
This article discusses the treatment of intersex infants, and particularly the re-assignment of genetic males as females. While many intersex children are genetically male, almost all of them are raised female. This means that many children who have XY chromosomes are being coaxed into female gender roles that nature may not have intended for them. This has been a common and accepted practice since the mid-1960's, however since the highly publicised failure of the gender re-assignment of
David Reimer
(aka the "
John/Joan
" case) there has been increasing and understandable concern about instances of
unsuccessful
sex re-assignment of intersex babies.
|
Prevalence of Intersex Infants
The Intersex Society of North America (
ISNA
) estimates that intersex infants account for one in every 1,500 to 2,000 births, i.e about 2,600 a year in the USA alone. Some statistics:
Not XX and not XY
|
one in 1,666 births
|
Klinefelter (XXY)
|
one in 1,000 births
|
Androgen insensitivity syndrome
|
one in 13,000 births
|
Partial androgen insensitivity syndrome
|
one in 130,000 births
|
Total number of people whose bodies differ from standard male or female
|
one in 100 births
|
Total number of people receiving surgery to “normalize” genital appearance
|
one or two in 1,000 births
|
Early genital surgery is a common and accepted practice, a 1998 article in Pediatric Nursing even suggested that doctors ought to consider it child abuse if the parents refused genital remodeling. Of those 2,600 infants at least 2,000 (the ISNA says 9 in 10) will have remedial genital surgery, including about 100 to 200 (4-8%) boy-to-girl pediatric surgical sex re-assignments such as John/Joan had. The later figure is supported by a long-term study of 700 intersex children which found that 40 (6%) had been sex re-assigned at birth.

Monica was identified as being male at birth and called Morten. She total assigned had RS , now in her mid-20's, doing her make-up. Girls practice this from as young as 2, and it presents an immense challenge to the about the transition boy-to-girl or man-to-woman. Their make-up is always vastly better a year after transition.
|
Sex Assignment
A persons male or female "sex" can be determined or judged by an extraordinarily large number of factors, and everyone's list differs somewhat, but here is my attempt:
| Chromosomal Sex: Male "XY" or female "XX" genes as determined by a karyotypic study (in rare cases there are other combinations). |
| Internal Sexual and Accessory Organs (Organs used for reproduction): The presence of male (testes) or female (ovaries) gonads, and male (e.g. vas deferens, ejaculatory ducts) or female (e.g. uterus, fallopian tubes) accessory organs. |
| Genital Sex (Organs used in mating): In particular male (e.g. penis, scrotum) or female (vulva - clitoris, labia majora etc.) appearing external genitalia, but also internal genitalia such as the vagina. |
| Hormonal Sex: Based largely upon male type androgen plasma levels, or female type oestrogen and progesterone plasma levels. |
| Secondary Sexual Characteristics: Physical attributes (other than the sexual organs & genitalia) that distinguish males (e.g. beard, Adams apple) from females (e.g. breasts, fat distribution) after puberty. |
| S |
keletal Sex: An assessment based upon
skeletal characteristics
influenced by sex (e.g. pelvis, shape of chin, height, size of hands and feet, robustness of bones ... ).
| Gender Role: The sexual role a person lives in, and the sex they are perceived as being by others. It has been defined as "A social status usually based on the convincing performance of femininity or masculinity". |
| Sexual Identity: The sex a person identifies with and believes they actually are. |
| Aristotelian sex: The role (male or female) adopted during love making. |
| Legal Sex: In the UK, since the |
infamous ruling
by Lord Justice Ormrod, this has effectively become irreversibly determined by the sex stated on the original Birth Certificate. The later can only be re-issued if a mistake was clearly made at birth, or in very
exceptional circumstances
.
|
An abnormality of the chromosomes (factor 1) is not strictly an intersex condition in itself, although it and hormone abnormalities are often associated with intersex cases. The criteria for determining the sex of the person to be registered are not laid down in the Births and Deaths Registration Act 1953, however, the practice of the Registrar General is to use exclusively the biological criteria: chromosomal, gonadal and genital sex. A baby is "intersex" when factors 1, 2 and 3 are not all normal male or female, or contradict each other. As initial assignment of sex is often made exclusively based on factor 3, and if the genitalia are normal appearing then it may be some time before it becomes evident that a baby is actually intersex, if the
sex of the infant
is then reassigned it will be extremely difficult to get the Birth Certificate changed.
|
 Katherine Connella was born Charles. She's the webmaster of www.intersexed.com
Katherine Connella was born Charles. She's the webmaster of www.intersexed.com
Factors 7 and 8 are commonly and unfortunately combined under "gender-role", but I prefer to keep them separate when possible. A particularly confusing but frequent use of the word
gender
is in the phrase "Gender Re-Assignment Surgery" (GRS). It's important to differentiate between physiological
sex
, and the social & mental
gender
, surgery can't ever change the later so "Sex Re-Assignment Surgery" (SRS) is a better, although still exaggerating, description of what surgery can achieve.
It is quite possible for the above factors to disagree and contradict, e.g. an intersexual person may have a female birth certificate, a male karyotype (XY genes), lack any internal female sex organs, have female appearing genitalia and sexual characteristics, live as a woman, but believe that she is really a man.
|
Sex Assignment and Re-assignment of Intersex Children
The sex assigned to a newborn baby is often only based upon the appearance of its external genitalia. If they appear to be "normally" male or female then an actually intersex babies may be unhesitatingly so assigned, and its real condition only discovered weeks, months or even many years later, e.g. at puberty.
|
Only if there are ambiguities in the genitalia is further investigation likely before a babies sex is assigned. When deciding the best sex to assign to an intersex child, the physician considers the following:
|
| a pelvic ultrasound (to check for the presence of female reproductive organs); |
| a genitourethrogram to look at the urethra and vagina, if present; |
| a chromosomal analysis (to help determine genetic sex: usually but not always 46, XX or 46, XY); |
| fertility potential of a female pseudohermaphrodite; |
| size and potential for growth of a penis present in a male pseudohermaphrodite; |
| ability of an internal reproductive organ to produce appropriate sex hormones for the gender; |
| risk of future health conditions (i.e., cancer) that may develop in the original reproductive organs later in life; |
| the actions of male or female hormones on the foetal brain; |
| the parents opinion or preference. |
Sex assignment is usually done within a few days of birth. However, occasionally a baby may be assigned to one sex at birth, but for various reasons the physicians later recommend its re-assignment to the other sex, e.g. because of the discovery of viable testes in a supposed baby girl. The earlier this re-assignment is done the better, and is very rare after about 24 months of age as it's considered that the baby's gender will be irreversibly set by then. The term "sex re-assignment" is also often used to refer to the deliberate legal and social sex assignment of a baby contrary to its chromosomal sex (e.g. assigning a "XY" baby as female), even if it was never actually assigned to its chromosomal sex.
|
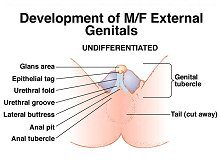
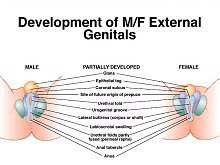
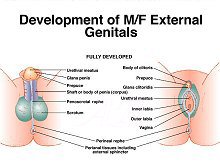
Normal development of male and female genitals (click to enlarge picture)
|
|
Doctors have a list of standards according to which they determine the "normality" of a newborn's genitalia, this includes two functional assessments of the adequacy of phallus size. Young boys should be able to pee standing up and thus to 'feel normal' during little-boy peeing contests; adult men, meanwhile, need a penis big enough for vaginal penetration during sexual intercourse.
|
The assignment of a genetically male baby as a girl is therefore often due to a badly damaged or undeveloped penis - surgeons can make a vagina relatively easily but it is hard to make a penis that is functional.
|
Boys are typically born with a stretched penis ranging in length from 2.9 to 4.5 centimeters (1.25 to 1.75 inches), with a urethra opening at the tip (rather than on the side or base of the penis) that releases urine, and a scrotum that contains testes. For new-born girls, clitoral length at birth typically ranges from 0.2 to 0.85 centimeters (0.08 to 0.33 inches). Those falling in between these two sizes will often have their organs shortened. A clitoris longer than 1 centimeter is considered unacceptably enlarged and may be shaved down purely for purposes of looking normal. On the other hand if the penis is less than 2.0 centimeters long, concern is often expressed about whether the boy will be a "boy".
|
 A pronounced "penoscrotal hypospadias" penis with the urine exiting the bladder from behind the penis.
A pronounced "penoscrotal hypospadias" penis with the urine exiting the bladder from behind the penis.
A penis less than 1.5 centimeters long and 0.7 centimeters wide is usually considered to be unacceptably short and inadequate for later sexual performance and thus deemed to be a clitoris, and he a "she". In this instance, although genetically "XY" male and perhaps with testes, the infant will be re-assigned as female and her "micropenis" surgically altered to become a clitoris. Such re-assignment is particularly likely if also the urethra does not open at the tip of the phallus, a condition known as hypospadias.
|
"If a baby has hypospadias, the urinary function will not be the same as other males," says Dr. Aydin Arici, a Yale-New Haven Hospital obstetrician and gynecologist who specializes in reproductive endocrinology, explaining why male babies with such a condition might be reassigned. "For example, that individual will not be able to urinate standing up."
|
Clearly the most important factors in the sex assignment of intersex children are: (i) achieving a "normal" appearance of the genitalia in the assigned sex; and (ii) sexual function. If a male's phallus is deemed unlikely to be able to "perform" adequately, then re-assignment as a female may become the preferred medical choice. But appearance and sexual function is not the only factor used in sex assignment - many laboratory tests are also done to determine the child's genetics and potential for fertility. In the vast majority of cases of significant ambiguity, however, a female assignment is made - perhaps sometimes for the sake of medical expediency. "It's easier to dig a hole than to build a pole," doctors are supposedly quoted as saying. But once a sexual assignment is made, it's effectively irreversible, especially if surgery must be performed.
|
Gender
With modern medical methods, establishing a normal female physical appearance for a genetically "XY" child is relatively easy. A far bigger problem is ensuring that the "girl" feels that she really is a girl and has a deep rooted female "gender".
|
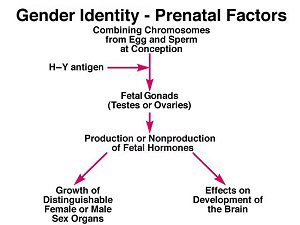
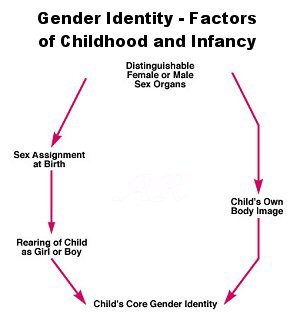
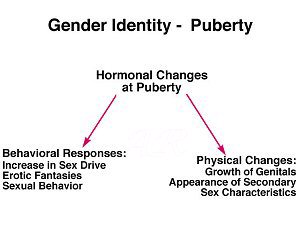
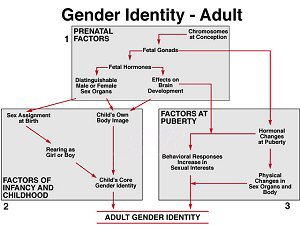
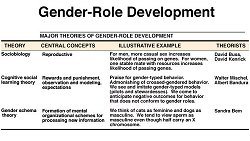 Three theories of gender development (click to enlarge)
Three theories of gender development (click to enlarge)
Establishing a gender identity is a process that most people take for granted, but that no one completely understands. Scientists and sociologists agree that traditional gender roles are in many ways socially constructed - girls learn to wear dresses and boys learn to wear pants. But no one seems to understand what makes a
transsexual child
raised in a female gender role embrace the male role as her own and vice versa. And no one can even begin to explain why many intersex children raised as one sex eventually migrate back to the gender that their genetics or their prenatal hormonal environment would have predicted.
|
Bill Summers, a professor of medical history at Yale who has studied the science behind gender and sexuality says "You have to learn somehow what it means to be a boy or a girl. You don't come born with this idea. But enough people say, 'I always knew I was a boy but I was raised as a girl' that I can't doubt they have these feelings".
|
John/Joan
, aka David Reimer. May he now RIP.
|
Professor Summers points to the work of John Money, a physician at Johns Hopkins University who became famous in the 1960s for turning a boy (Bruce Reimer) with a botched circumcision into a girl (Brenda) - the so called 'John/Joan' case after the names used by Money. Money initially declared victory, but his work was later undermined in a landmark
study
by doctors Milton Diamond and Keith Sigmundson which revealed that the girl grew up with a masculine gender identity anyway. Summers says "The whole idea that given hormone treatment and the right social environment, you can determine gender identity. It's not really quite so simple". 'Joan' herself proved the point, 'John' ending his tragic life in 2004 with suicide .
|
Nevertheless the 'John/Joan' case is actually fairly unusual as John was reassigned female as Joan at just seven months age, and there are apparently numerous cases of
successful
gender re-assignment at this age. Indeed, since the 1960's it has become accepted practice that young boy babies with genitalia problems can be gender re-assigned as female if this will later allow them a normal sex life as woman, which they could not have as a man. The American Academy of Pediatrics has established a
policy
that states "children whose genetic sexes are not clearly reflected in external genitalia (i.e. hermaphroditism) can be raised successfully as members of either sex if the process begins before the age of 2 years.".
|
However the authoritative John Hopkins Children Hospital has recently become slightly more
cautious
, saying: "While we recommend that sex assignment be postponed until after a diagnosis is made for a newborn with an intersex syndrome, older infants or children will have already lived as either a boy or girl regardless of diagnosis. In such instances, it is usually best to continue with the original sex assignment because such a change is often unsuccessful if it occurs after the first 18 months of life. We feel that sex re-assignment within the first month of life is most likely to be successful if such a change is determined necessary by parents and doctors. For most older children, a re-assignment should only be considered if desired by the child."
Some scientists claim that subtle cues from parents contribute to divergent gender identities in re-assigned intersex children. But studies of intersex siblings who are both genetically female, are both raised as girls in similar environments and both unexpectedly masculine at puberty show that one sibling might embrace a new masculine identity while the other one rejects it. While social cues were undoubtedly important, the children's identity must have at least partially come from something inside of them. Since both children were genetically female, this identity could not have been entirely genetic.
Other scientists believe that sex hormones acting upon the brain during development play a big role. This seems to be true for establishing both gender identity and future sexual orientation. But scientists still cannot explain how hormones could make someone feel like a member of a particular sex, as so many intersex people say they do. The bottom line: We just don't know where gender identity comes from, but it is unlikely that either biology or society operates independently from the other. Given this mix, the danger inherent in operating on a non-consenting intersex infant increases manifold. If surgeons turn a genetically male child with testes and an "inadequate" penis into a girl, they not only destroy his future fertility and sexuality, but may compromise his chosen gender identity as well.
|
"How does [intersexuality] affect the brain? I don't know," Boney admits. "But we shouldn't change the genitals because we just don't know if the child will want them later."
|
Gruppuso cites the example of one of his patients, an XY intersex child raised as a female, who decided at adolescence to transition to a male. "The traditional approach assumed that assigned gender would be accepted by the patient when he or she grew up, as long as the assignment was accepted by the parents in an unambiguous way. We now have reason to suspect that assigned gender may not be accepted by the patient later on," he says.
|
Overall, the evidence from matched control studies of gender re-assignment in infants who had ambiguous genitalia indicates that the destiny of gender in early childhood is locked at a critical period similar to imprinting in lower animals; this period is partially determined by thyroid hormone levels. The window of opportunity closes between 18 and 36 months; the same period in which language acquisition occurs. Both windows are probably effects of myelination, dendritification, and vascularization of the central nervous system completed at about 18 months. In children brought up contrary to their biologic sex due to the presence of ambiguous genitalia at birth, the further away from this critical period, the more difficult is the attempt to reassign gender.
|
Female Sex Assignment Procedure
Given the above gender considerations, female re-assignment surgery is typically done within days of birth and less than 9 months is considered optimal. The John Hopkins Children Hospital
advises
that "Generally speaking, it is better to try to obtain full correction of the genitalia before the child is two years of age, when he will be less aware of the problems related to surgery ... accepting that mild complications may occur later in life." This approach is felt to minimize the trauma of the operations, also female appearing genitals help psychologically to reinforce the girls female gender and will prevent undesirable "locker room" problems at school, etc.
For good or bad, a "photo shoot" of this intersex woman has become famous long after her death. Genital surgery was not an option for her.
|
Gary Berkovitz, director of pediatric endocrinology at the University of Miami School of Medicine, explains the early re-assignment procedure for female assigned babies as follows: "We remove the testes because they would make testosterone and virilize a girl. The phallus is recessed. Current techniques emphasize maintenance of innervation, and experimental evidence indicates that sensitivity in the new clitoris is preserved. However, none of the children has grown to adulthood yet to see if it works. The new techniques are very different than what was done 30 to 35 years ago. .... Hormones are part of the picture too. We initially try to re-create a normal puberty, give a little estrogen at first, then progesterone. The girl won't bleed because there is no uterus, but she can have normal cycles. Often it is possible to do this with birth control pills as the estrogen supplements. Breasts develop too, given appropriate hormonal stimulation."
Further plastic surgeries during puberty usually complete the transformation, with the external female genitalia being "touched up" and a vagina created when the young woman is ready to begin her sex life. For the vaginoplasty, tissue from the child's colon is transplanted and fashioned into an artificial vagina that is capable of receiving a penis during intercourse. The vagina must be dilated either through regular intercourse or with an artificial dilator up to several times a day, sometimes for years, to ensure that it remains open.
Doctors usually don't perform vagioplasties until the child reaches adolescence, but they are sometimes performed at a young age, requiring parents to perform the dilations on their children an act that would normally be considered sexual abuse.
Historically the results of genital surgery have often been unsatisfactory - loss of sensitivity, pain on intercourse and unacceptable appearance being common. But surgeons are adamant that techniques have much improved in the last ten years and that the final results of surgery and hormonal treatment are almost always very successful, the young woman presenting an undoubtedly female physical appearance even under the closest examination, as well being sexually functional.
Research
Since the unfortunate outcome of the John/Joan case was revealed there has been further research in to the long-term effectiveness of early sexual re-assignment. The results have raised more concerns and shown that John/Joan was not a unique incident.
One study of 27 boys reassigned and raised as girls found that 3 now live as males, an unsatisfactory 11% failure rate - although the same research found that sex re-assignment was apparently successful in the vast majority of subjects.
|
A study of 6 intersex woman found that all cases the results of the genital surgery they had undergone as babies left a lot to be desired, even after subsequent remedial operations the appearance of their genitals was often still judged unsatisfactory - it is indeed to be hoped that surgical techniques have now greatly improved.
|
More positively, one study of 85 people ranging in age from 21 to mid-60's with various intersex conditions (including a 6 patients born with micropenis who were raised as women) showed that almost all of the patients were content with the gender in which they were raised. All but two showed a gender identity and gender role in accordance with their gender of rearing.
|
Sexual Orientation
One of the interesting phenomena of the intersexual and transgender political movements is the fact that the majority of the "female" activists seem to identify themselves - sometimes very forcefully - as lesbian. This can be confirmed by just a cursory examination of autobiographies and personal stories on relevant websites. Taken at first appearances, the distribution of sexual orientations found in intersex women would seem likely to differ remarkably from the sexual orientations found in natal "XX" women - an overwhelming 95% of whom consider themselves as being heterosexual even in this sexually liberated age.
However, while the limited available medical evidence does suggest that a lesbian or bisexual sexual orientation may be more likely in a woman who was sex re-assigned as a infant than for a natal women, those with a primarily heterosexual attraction to men are still by far in the majority. The actual situation is therefore being somewhat misrepresented in the public perception.
This may in fact be a result of a deliberate assimilationist philosophy by many women. Boy-to-girl intersex children who settle well into their assigned gender and grow up identifying themselves as heterosexual women tend to assimilate to the point of entering so-called "normal" committed relationships with men. Those who identify as lesbians find themselves marginalized from mainstream society to some degree because of their homosexuality. On the other hand the psychosocial realities facing a sex re-assigned woman involved in a relationship with a man tends to pull her away from open activism: for example social stigma attaches to an alleged heterosexual man once it becomes known that his girlfriend or wife was born a male. Additionally, painful childhood experiences will often dissuade her from wanting to talk to her partner about her "secret", and she may feel that doing so will break the relationship. In the balance between personal happiness and political activism, the successfully sex re-assigned woman, perhaps married with a good career and adopted children, will usually choose happiness.
 Thea Hillman - poet and intersex activist
Thea Hillman - poet and intersex activist
Differing View Points
Intersex organizations such as the Intersex Society of North America (
ISNA
) and the UK Intersex Association (
UKIA
) are generally against the sexual re-assignment of babies and (in particular) any early non-essential feminizing genital surgery. [Please go to their sites for more information on this.]
Many activists believe that genital surgery on infants should be considered despicable and cruel rather than routine. Their experience is that intersex genital "mutilation" and other medical management of intersex children results in post-traumatic responses similar to other forms of childhood sexual abuse. They believe that an intersex person should be left able to make an informed decision herself on whether to have genital surgery, at the appropriate point in her life. [Another possible route some times advocated is for the intersex child and his/her parents to make decisions together sometime before adolescence.] Meanwhile, doctors can assign a temporary gender without surgery, based on medical tests and physical appearance, with the understanding that the child may wish to transition to the opposite gender later in life. Interestingly, the ISNA does not support any attempt to break down the binary system of gender and allow for a "third sex." It calls such a designation impractical and arbitrary.
However, there are still supporters of early surgery and sex-reassignment. Despite the undoubted mistakes made in the past, the case for a "no early surgery" policy is still disputed and in practice is a hard demand to meet. Most physicians do not consider what they are doing to be wrong and still recommend surgery for intersex births, while many parents feel desperate to "fix" their children. Also, it should be remembered that while there are now many well documented and sometimes well publicized instances of the problems caused by early genital surgery on intersexual children, and the child's later rejection of their assigned sex, statistically these still form only a very small proportion of the total number of treated intersex infants, as is shown above. There are assuredly many cases where a sex assignment / re-assignment and associated early genital surgery can be judged, even after hard questioning, to have been extremely successful. Certainly not everyone - even those who work with intersex people - believes that genital surgery is necessarily inherently evil. Many specialists argue that the current Model of Care for intersexual children actually works quite well.
"If our study shows that the vast, vast, vast majority of people are in fact happy with the gender alignment that is given to them, then I'd actually ask the question 'Well of the few that we've made the wrong gender assignment to, could we have retrieved that situation earlier, but how different is the rate of that occurring to trans gender, transsexual issues occurring in the rest of the population?'," argues Dr Sonia Grover, a gynecologist at the Royal Children's Hospital in Melbourne. In our society we tolerate that some males feel like women inside. "So we should, and I think we need to have the broad-mindedness and openness to do the same in our patients with medical conditions."
 Joella (formerly Joel) Holliday, age 10 (left) and 20. She was re-assigned as a girl at 12 months due to major genital defects but only got a new female birth certificate when age 12, when started taking female hormones. Happy as a girl she hopes to one day meet Mr Right and adopt.
Joella (formerly Joel) Holliday, age 10 (left) and 20. She was re-assigned as a girl at 12 months due to major genital defects but only got a new female birth certificate when age 12, when started taking female hormones. Happy as a girl she hopes to one day meet Mr Right and adopt.
Dr Grover believes that surgery can be more successful if it is done in children rather than at a later age, because the patient is smaller. "It's not necessarily easier for me to make the corrections that I've watched the pediatric surgeon here in Melbourne do with relative ease in little children," she said. "I'm also conscious that it's counter to what other people are saying elsewhere in the world, that we shouldn't be doing it on little kids, and we should be doing it when they're older. I'm not sure. I'm not sure that I'm failing in terms of sexual function outcome but I feel like I have to work much harder to get a good outcome than the paediatric surgeon, John, who does it as a baby." she explained.
"The ISNA is particularly unhappy about the surgeries. But this is a skewed population. That's why those people join the ISNA, because they are upset," says Rosario, the UCLA sexologist and child psychiatrist. While some ISNA members hope that intersex children will be allowed to make their own decisions about genital surgery once they reach adolescence, Rosario is unsure that intersex teenagers can make decisions any better than their parents can. "Teenagers are freaking out about pimples-how can they even begin to think about correcting their genitalia?" he says.
The arguments have been summarized by Ian Aaronson, a urologist at the Medical University of South Carolina. "There are presently two points of view" says Aaronson. "The first - do nothing, let patients assign themselves, no surgery - is held by psychiatrists who have had to deal with patients who have, in retrospect, been badly handled - John/Joan, for example. This is countered by many physicians who believe, all in all, their patients are doing quite well."

The brutal reality - a young intersex child assigned as a boy. His vagina is about to be removed and a penis created.
|
The Arguments for Early Surgery:
| Children come to know whether they are male or female before the age of two. Early surgery and, if required, sex reassignment helps both socially and psychologically to create a clear gender identity. |
| It helps reassure disturbed parents who want their child to look normal. As it's often easier to construct normal looking female rather than male genitalia, this may require sex re-assignment of the child. |
| If surgery is undertaken by experienced surgeons using the latest techniques then the results should be excellent in terms of vulva appearance, clitoral sensitivity, and vaginal depth. |
| Some surgery can be more successful if it is done in children rather than at a later age. |
| The surgery may be medically recommended, e.g. to prevent recurrent urinary tract infections, |
The Arguments for Delay:
| Early genital surgery is often for purely cosmetic reasons, it's rarely required for medical or health reasons. |
| The person with ambiguous genitals should be involved in any decision to have "corrective" surgery, and should not have it imposed upon them. A significant number of intersex people, when they become adults, complain that they had their genitals restructured as a child in ways that they don't approve of. |
| Historically, many assigned girls have been the victims of poor quality surgery performed by inexperienced surgeons, e.g. resulting in an unnatural looking vaginal opening, lack of clitoral sensitivity, discomfort during intercourse. |
| Children who have had early surgery need to have their genitals regularly examined during childhood, which can have a profound effect on their attitude towards sex. |
| The few available studies show a very high success rate for XY babies born without penis who are raised as boys, but a somewhat lower rate for those surgically reassigned and raised as girls. |
| The removal of gonads, the testes or ovaries, also removes their capacity to produce hormones, which raises issues when the patient reach's their adolescent years - it's critical that they take their hormones puberty but teenage rebellion is a problem. |
| The high profile publicity surrounding the "John/Joan" case, et al. |
Intersex or Transsexual?
In recent years there has been a proliferation of male-to-female transsexuals claiming that they have had to start taking female hormones due to a serious medical problem, by implication this is often an intersex condition. Unfortunately - without detailed medical records - it is often impossible to differentiate between MTF transsexuals born as 'normal' boys, and those with intersex conditions.
Eva Robins
is perhaps the most famous instance of this.
Another typically confusing case is a
Lady Colin Campbell
. She was born in 1949 with genital deformities, the doctors advise her parents to register the baby as male, and she was christened 'George William Ziadie'. Although being bought up as a boy, by age 3 she preferred to play with dolls and sew. At age 11 she was sent to a boys only school but at age 13, realizing she was attracted to boys, she secretly consulted her mother’s gynecologist, who was sympathetic to her plight and may have given her Estrogen injections. By her late teens, she was living openly as a girl and calling herself Georgia. Age 18, she moved to New York to study fashion design and began modeling and dating men, making her desperate to claim “my true identity”. Whilst there, her grandmother paid the $5,000 for "sex change surgery ... No one ever faced the knife more eagerly than I – you would have thought I was going on a wonderful cruise.” When aged 21, she somehow managed to obtain a re-issued birth certificate giving her name as 'Georgia Ziadie', and (far more critically) stating her sex as being 'Female'. In 1974, she married Lord Colin Ivar Campbell, the son of Ian Campbell, 11th Duke of Argyll; they were divorced in 1975 (Lord Campbell claiming that he was unaware that his wife was a "transsexual") but she continues to use the title and surname from the marriage.
The Future
The bottom line is probably that we don't have good enough research to make good decisions.
|
Cheryl Chase, founder of the NATFI
|
The studies that have been done suggest most intersex people are satisfied with the gender they were assigned, though maybe not with their equipment.
However, the ISNA's propositions seem to be gradually gathering support. The North American Task Force on Intersexuality (NATFI) was recently formed, and this organization hopes to put some of the ISNA's ideas into practice through education and medical reform. NATFI plans to establish guidelines for the medical management of children born with ambiguous genitals but not until first completing multi-center follow-up studies of a range of intersex patients to determine their psychosexual and functional outcomes. Those studies should take about three years.
While far more work needs to be done before it can be certain that early genital surgery on an intersex child is always the wrong choice, surgery is undoubtedly becoming less common for "minor" cases of genital abnormalities, this revised positioned being undoubtedly assisted by the fact that in the last decade the diagnosis and treatment of genital disorders has advanced dramatically.
John Hopkins's
John P. Gearhart, who directs the Department of Pediatric Urology points out that debating a case like John/Joan's is really a moot point, today such a child who tragically loses his penis would certainly be raised as a boy and would undergo penile reconstruction surgery at age 10 to 15.
There is also an increasing reluctance by physicians, possibly in part worried by the negative publicity, to reassign a physically intersex but chromosomal male babies as female. Even when sex re-assignment seems the best option, many specialists may now prefer [rightly or wrongly] to delay any major genital surgery until puberty when it's become clear that the girl has adjusted well to her assigned social gender and has begun taking feminizing estrogen.
Possibly the last words on this page should be left to an echo from a defunct intersex support site: "Intersexual's who are subjected to neonatal surgery undergo that early physical trauma and resulting lifelong trauma on many levels, [while] intersexuals who miss early surgery often grow up alone and confused... and often abused", but I hope that is an excessively bleak and depressing point of view in many cases.
Useful Links
Some Sources


{kind=link}
{kind=link}
{kind=link}